By this time you have received a diagnosis based about the biopsy findings. You know no matter if or not you've tumor. Your diagnosis was produced by the pathologist-the only member of your diagnostic team whom you most probably will not meet, consist of information on regardless of no matter whether or not cells are present, and the character from the cells which are observed under the microscope. A surgical pathology report may be within the form of the template or freely dictated, but either way it ought to include particular details. Don't just study the summary of the findings on the finish from the report.
Study and fully grasp the physique from the record. Look on the sample surgical pathology record at the end of this chapter. Note the separation of gross findings from microscopic findings. Though they are unique, each are very important towards the final diagnosis. The "gross pathology" might be dictated by a several pathologist from the 1 who signs the report, considering the gross pathology is done the day the specimen arrives in the pathology laboratory the tissue isn't study until it has been examined below the microscope by the pathologist who dictates the microscopic findings. The final surgical pathology report might not be typed and signed until days later.
The vital information you will need to glean from the gross pathology is the size, place, and character from the specimen muscle as a complete, and the size, place, and character from the tumor (if there is any) that may possibly be contained inside it. Do not confuse the two. The larger dimensions of the specimen as a entire are not the dimensions from the cancer. The size from the cancer has important implications for the "stage" from the tumor. If tumor is diagnosed within the specimen, the further description of the muscle, as set forth in the gross pathology, becomes essential, such as the location of the cancer within the specimen as aentire. For example, a pathologist frequently can make the diagnosis of inflammatory breast cancer when he or she sees, beneath the microscope, cancer cells in the lymphatic ducts of the skin-the "dermal lymphatics."
When the tumor is situated on the edge from the specimen and is cut through, a reexcision will be vital. The gross pathology has told the complete story. The microscopic pathology to come will simply confirm that the margin is very good. The color and also the consistency of the tumor inside the specimen are also relevant, in that they may well characterize the tumor. Right after dictating his or her findings, the pathologist who carries out the gross pathology will cut some of the tissue into modest pieces and put them into "cassettes," porous holders of the fragments. The cassettes are submerged in a fluid that preserves the tissue.
Please note that the pathologist cannot examine just about every cell in a core needle specimen, or inside the larger specimen of an open biopsy. He or she may well "bread loaf" the tissue by cutting it into slices like a loaf of bread and putting representative sections into cassettes. The remainder of the specimen is retained in jars containing preserving liquid, so that if there are any questions concerning the pathology, further muscle can be examined. Legally, the pathology department will need to maintain the preserved tissue for a specified period nothing will need to be thrown away at the time of the procedure. Suitable soon after an appropriate time, laboratory technicians prepare the preserved muscle further for the pathologist who will carry out the microscopic examination.
They location quite thin sections from the tissue on glass microscope slides, stain them appropriately, and cover them. The pathologist reads the slides below the microscope and dictates the "microscopic examination" portion from the record. The concluding summary provides the gist of the gross and microscopic findings. The most normal breast region cancer is called adenocarcinoma. The term is truly a composite: "adeno" describes the tissue of origin of the cancer "carcinoma" is honestly a fancy term for cancer. Thus, an adenocarcinoma is a tumor of glandular origin. And a breast area adenocarcinoma is really a breast area cancer of glandular origin.
The distinct muscle where the breast region cancer has originated is either inside the duct program from the breast (when it is recognized as ductal adenocarcinoma or, a lot way more typically, ductal carcinoma) or in the lobules (the part of the breast method precisely exactly where the milk is produced). Lobular carcinomas, when invasive, possess a life expectancy related to that of invasive ductal carcinomas. Despite the fact that they might have different characteristics, the two are subjected towards the very same therapy. (You should be conscious that invasive lobular carcinomas often are not visualized on screening mammograms basically because, it is believed, their outside edges have alot more tendrils and are not distinct.)
Each ductal and lobular carcinomas are treated differently when they are noninvasive than when they are invasive. A non invasive ductal carcinoma (otherwise known getting a DCIS, an acronym for ductal carcinoma in situ) consists of a distinctive treatment path from that of the lobular carcinoma in situ, LCIS. The record dictated from the pathologist is typed and submitted to him or her for approval and signature. Lastly, it is conveyed to you. You are in a position to see why it takes a few days to problem the pathology record, and a quantity of a lot even more days till you get the outcomes. Your physician might possibly wish to shorten the time involved by phoning the pathologist and acquiring an oral record.
But should you then get the report from your physician, who did not see the muscle beneath the microscope, it is undoubtedly feasible for error to creep into the transmission. Whenever you obtain the formal record, study all of it, not just the summary. If you do not understand the particulars, ask your physician to clarify them. Pathologists ought to know all concerning the tissue they are handling, such as the "natural history" (untreated history) from the tumor. The report will contain the answers to three big concerns: Do you have cancer? If so, what kind is it? And particularly, is it invasive or noninvasive? The pathologist's answers will have profound consequences for your remedy. If the margin is positive, the pathologist will need to be able to say how very good it's.
As you can see from Figure 6, the margin could be "grossly" positive (numerous, lots of cancer cells are there) or "diffusely" decent (only a relatively few cells can be observed). Obviously, when the yolk is off center, at the edge from the white of the egg, and is cut via, the margin will be referred to as grossly positive. Truly, if the tumor has been cut by way of, a major number of cancer cells will remain in the tumor bed (the remaining muscle in you). Even although it is essential for the team to know when the margin is grossly or diffusely excellent, the bottom line for you is that if the margin is recognized as positive, extra surgery-a reexcision of the margin of the tumor bed-have to be regarded as. If the pathologist's report proper right after your biopsy describes cells in the lymphatics of the skin, you possess a diagnosis of inflammatory breast cancer. If that specialized cancer is treated like plain old breast location cancer (POBC), the outcome could be disastrous.
Any suspicion of inflammatory breast location tumor need to be followed up, with a second opinion from an additional pathologist or oncologist if vital. As opposed to the remedy for POBC (surgical therapy, chemotherapy or hormonal therapy, and radiation), the sequence of remedy for inflammatory breast cancer is chemotherapy or hormonal therapy 1st, then surgery, and then radiation. If inflammatory breast tumor is treated getting a mastectomy on the outset, the cancer cells inside the dermal lymphatics are cut by way of on the time from the initial surgery and can spread all over the chest wall. Soon thereafter, tumor nodules can seem on the chest wall en curasse-covering the entire chest wall. This progression spells disaster for the patient.
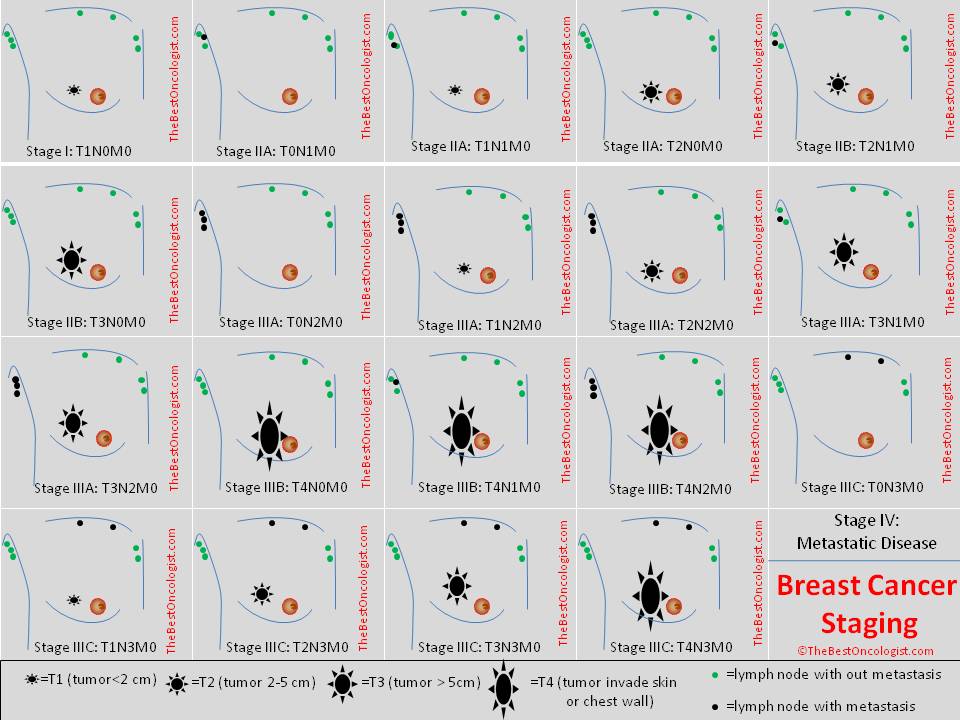
If chemotherapy or hormonal therapy can render the dermal lymphatics no cost of tumor, you will acquire two outcomes. Initial, the peau d'orange look from the breast region skin can disappear and, second, surgical remedy could be carried out safely. On the very same time, the systemic treatment affects the huge central mass of tumor and makes it much smaller, and subsequently surgically amenable to remedy. The pathologist has nonetheless one more role: to give the tumor a pathologic stage. This last and essential staging includes a substantial bearing on your future. The pathologist in no way creates formal remedy recommendations, because the pathologist is not a treating physician.
The remedy team makes therapy recommendations. Only the patient makes remedy decisions. The pathologist may possess a robust opinion about what the remedy ought to be, but it is not stated in the pathology report or in any formal setting in which the pathologist participates (for example, at a tumor board-about which you will hear a lot more in a moment). If the disease or tumor diagnosed is rare, the pathologist could comment appropriately inside the pathology record. Patients are frequently pleased to have their case presented to a tumor board. They picture that physicians with distinct specialties will especially meticulously evaluate their case. The operative word is quite cautiously. Optimally, the slides should really be presented by the pathologist assigned to the tumor board as well as by the presenting doctor. Presumably the pathologist has had time to evaluation the slides beforehand.
Similarly, the x-rays should really be evaluated prior towards the tumor board meeting and presented from the assigned radiologist. If the slides and x-rays are meticulously reviewed and presented, the role from the tumor board can be highly meaningful. Regularly, still, the films or slides are not present. Or the pathologist or radiologist is absent. Or the specialists have not had sufficient time to assessment the slides or films. Often the attending doctor is seeing the slides for the very first time. In such hit-or-miss circumstances, the board's recommendations may possibly not be definitely thoughtful or they could be biased in favor from the presenting physician.
Even if the tumor board is nicely organized and nicely prepared, the circumstance regularly is presented rather easily. The pathologist, the radiologist, and also the physicians on the board have small chance to think about the scenario, the patient is not seen, and the recommendations may be tainted from the presentation. There is no substitute for seeing and examining the patient and taking sufficient time to believe about the scenario appropriate after reviewing all the records, films, and slides. Tumor board recommendations are just that-recommendations. They need to never ever be accepted as definitive treatment choices. Your remedy team is responsible for explaining your treatment choices to you, and only you are in a position to make a decision what remedy you'll have.